Vulnerability is hard, and it’s scary
And it feels dangerous
But it’s not as hard
Scary or dangerous
As getting to the end of our lives
And having to ask ourselves
What if I would’ve shown up?
Brené Brown
The Call to Courage
Vulnerability is hard, and it’s scary
And it feels dangerous
But it’s not as hard
Scary or dangerous
As getting to the end of our lives
And having to ask ourselves
What if I would’ve shown up?
Brené Brown
The Call to Courage
 “Many of the people I admire lead lives that have a two-mountain shape.
“Many of the people I admire lead lives that have a two-mountain shape.
…
If the first mountain is about building up the ego and defining the self, the second is about shedding the ego and dissolving the self. If the first mountain is about acquisition, the second mountain is about contribution.
…
Over the past few decades the individual, the self, has been at the center. The second-mountain people are leading us toward a culture that puts relationships at the center. They ask us to measure our lives by the quality of our attachments, to see that life is a qualitative endeavor, not a quantitative one. They ask us to see others at their full depths, and not just as a stereotype, and to have the courage to lead with vulnerability. These second-mountain people are leading us into a new culture. Culture change happens when a small group of people find a better way to live and the rest of us copy them. These second-mountain people have found it.”
More on The Moral Peril of Meritocracy: Our Individualistic Culture Inflames the Ego and Numbs the Spirit. Failure Teaches Us Who We Are. By David Brooks via The New York Times. (Thank you Tina for sharing!)
Image of Mt. Rainier at Dusk via J. Ashby.
#MeaningfulConnections #MustRead #GameChanger
Greetings! Our Department of Family Practice is currently exploring the clinical placement model and environment. Given this, our Abbotsford-Mission site took the opportunity to use the design thinking process to consider how the clinical learning setting would look if it were to:
1. Support the inclusion and practice of medical students, residents, clinical educators, and their staff, and;
2. Offer patients interdisciplinary, team-based care.
During our Academic Half Day, we assembled in teams of 2-3 and went through a series of steps including:
1. Create a Blueprint: Plan and draw out the space. Describe the objectives of each area and services provided.
2. Design a Narrative: Describe the experience and transition of patients, learners, and educators within the environment.
3. Illustrate the Accommodation: Describe the activities, resources, and number of users that may be accommodated.
Here are the results of our three teams:
TEAM ONE: Patient-Centred Sanctuary: Music School Model
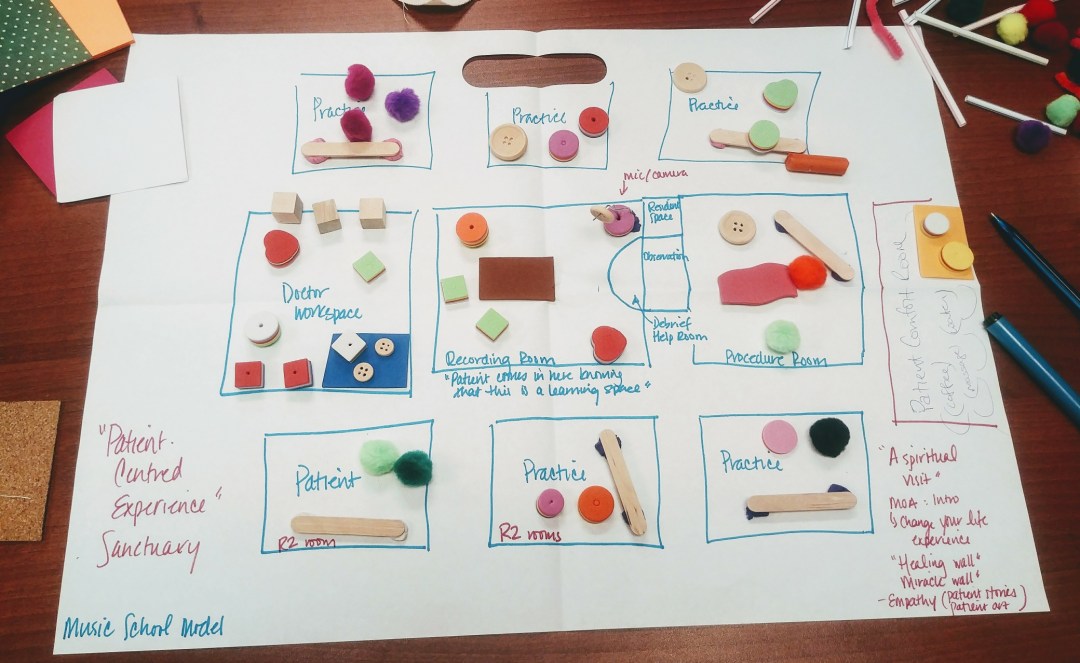
A music school is the inspiration behind the physical design and layout of the space. The clinic’s objectives include offering patients a sanctuary that is safe and comforting in addition to providing learners an environment that is centred on education and patient inclusion. The patient enters the space on the right side and is greeted by the medical office assistant (yellow rectangle).
The patient area is surrounded by “empathy” and “healing” walls. The “Empathy Wall” contains patient stories and art. In this room they are offered services such as coffee, water, massage, and aromatherapy. In the middle of the space is the “Recording Room” (brown rectangle) where the student and/or resident, preceptor, and patient explore learning. Patients invited into the Recording Room are intimately involved in the learning process and assist both preceptor and learner in delivering care. There is an “Observation Room” directly attached to the right of the Recording Room for learners, educators, and patients to observe, provide constructive feedback, and debrief.
Above the Observation Room is a small private “Resident/Student Space” designated for computer work, note taking, etc. To the right is a large “Procedure Room” (pink rectangle) that allows for the team to watch and engage with both spaces. To the left of the Recording Room is the “Doctor Workspace” (blue rectangle) that offers an open concept setting allowing for physicians to converse on patient, teaching, and learning matters. Surrounding the Recording Room are a series of “Practice Rooms” designed for R2s who require less observation in their work with patients and more hands-on experience.
TEAM TWO: Patient Education & Empowerment Model
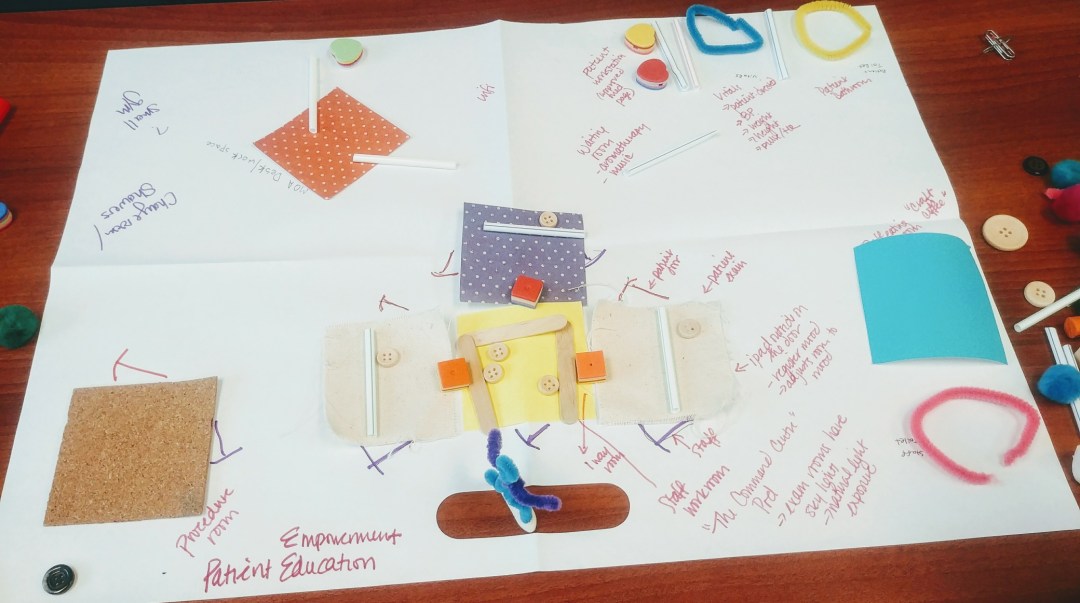
The objectives of this clinic include empowering and educating patients as well as supporting physician wellness and learning. Patients arrive at the top centre of the layout where they are greeted by the medical office assistant (represented by orange polka-dot square). As the patient enters the space, they experience aromatherapy and light music.
To the right of the room, there are a series of “Patient Workstations” (heart-shaped cushions) and wifi that offer access to patient-centred educational websites and resources. Once greeted and checked in, the patients are then asked to head into the room on the right that educates them on taking their own vitals including blood pressure, heart rate, weight, and height. Next to the “Vitals Room” (blue pipe cleaner) there is a “Patient-Dedicated Bathroom” (yellow pipe cleaner) to the right of this space.
In the centre of the office is the ”Learning/Command Centre Pod” (yellow, white, purple polkadot squares) that has a series of “Patient Exam Rooms” (white squares) where students, residents, and preceptors meet with clients. As patients enter the room, they come upon an iPad located at the door that registers their mood and responds by adjusting the exam room’s lighting, scent, and music to provide greater patient comfort. Each room is outfitted with one door for staff and one door for patients as well as a skylight for natural light.
The “Staff Workroom” (yellow square) is where physicians and learners can convene to discuss their experiences. There are one-way mirrors that connect the Staff Workroom to the surrounding patient rooms allowing for observation. To the right of the Learning Pod, is the dedicated “Staff Bathroom” (pink pipe cleaner) and “Meeting Room” (blue square) serving treats and craft coffee. To the left of the Learning Pod is the “Procedure Room” (cork square) again offering two separate doors for staff and patients. In the top left-hand corner, there is the “Staff Gym” and “Change/Shower Room” that encourage employee health and wellness.
TEAM THREE: Patient-Family Oriented Model
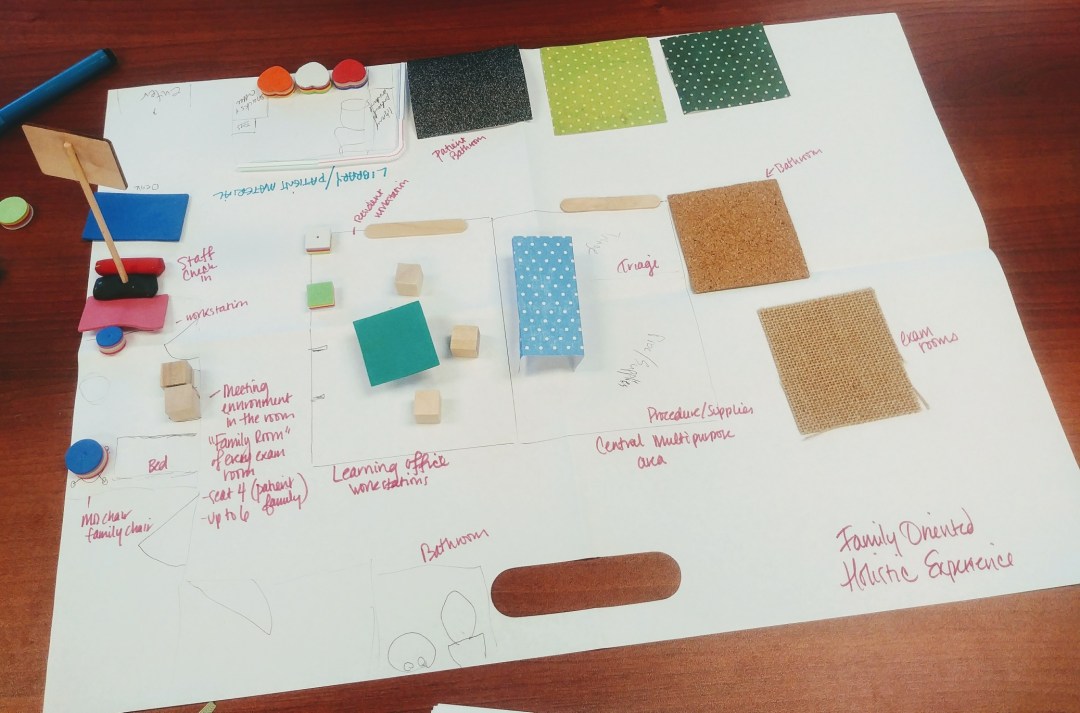
The main objectives of this clinic include creating an inviting and inclusive environment for the patient and the patient’s family members. The residents working on this space discussed the increasing presence of family members at their clinics and felt the need to accommodate them.
The patient enters the setting from the top left-hand corner (blue rectangle) and is greeted by a medical office assistant at the front. On the right side, they have access to comfortable seating (heart-shaped cushions), a library, snacks, coffee, and toys for the kids. To the right of the “Patient Learning” area is the “Patient Bathroom” (black square). On the far left, the patient enters the exam room, now identified as the ”Family Room” (pink rectangle) where patients and their family are encouraged to make themselves at home. These rooms are fairly large in that they can accommodate for up to 4-6 people.
In the centre of the space is the “Learning Office” (aquamarine square) outfitted with a series of “Workstations“. To the right of that room is the “Procedure/Supplies Room” (light blue polkadot rectangle) empowering and educating both learners and the patients on the procedures being performed. Surrounding the space are varied “Exam Rooms” for learners and educators to see patients and debrief their experiences.
In summary, this exercise emphasized that there are several ways to think about a clinical learning space that is designed to address a variety of patients’ needs while also accommodating for one’s learning and development. All the models illuminate the creativity and genius of our Residents as they take their experiences and ideas and articulate them on paper. I hope this provides others the inspiration to tinker with their clinical space and consider other alternatives and perspectives as to how people experience their environment.
A big thank you to our Residents for participating and providing your insights and thoughts on how we can design a clinical learning environment for the present and future of healthcare.
Warm regards and have a great weekend,
Jacqueline
#EcologyOfCare #DesignThinking #Ideate #Prototype #ClinicalPlacementModel #ClinicalLearningEnvironment #HumanCentredDesign

“The Potlatch is a high‐context (ancient, culturally and spiritually informed) approach designed to apply intercultural/transformative learning concepts necessary for witnessing greater intergenerational learning and success. At the micro level, the method can be used to engage your students and to design your lessons plans and rubrics; at the macro level, its utility can also serve to respectfully engage community scholars to help indigenize your institution (Wilcox et al. 2008). In this article, we model the ways in which we create inclusive teaching spaces by incorporating our Indigenous languages, storytelling, and ways of knowing and learning into our courses and teaching approaches.”
More on Looking Back to the Potlatch as a Guide to Truth, Reconciliation, and Transformative Learning (2019) by Justin Wilson and Aaron Nelson‐Moody (Tawx’sin Yexwulla).
A big thank you to Cheakamus Centre for hosting this lecture on Potlatch as a Methodology facilitated by Justin Wilson and Aaron Nelson‐Moody (Tawx’sin Yexwulla).
Warm regards,
Jacqueline
#CheakamusCentre #Híɫzaqv #Skwxwú7mesh #Potlatch #Methodology

CALL FOR SUBMISSIONS: UBC MEDICINE’S 14TH ANNUAL ART SHOW
UBC Medicine’s 14th Annual Art Show is now accepting submissions! We are accepting art submissions from students, residents, alumni and faculty members. We welcome all pieces of visual art of all skill levels, including but not limited to paintings, illustrations, sketches, prints, photography, sculptures, installations, sketchbooks, etc. Works must be framed and ready for hanging, or otherwise ready for presentation. The submission deadline is Saturday April 20th, 2018 at 11:59 PM. Click here to submit!
The Art Show is organized by Arts in Medicine and is an exhibition of visual arts by members of UBC’s medical community, held each year at the Medical Student and Alumni Centre (MSAC).
The Art Show itself will be held Sunday, April 28th at the Medical Student and Alumni Centre (MSAC). The show will be open from 12-7PM, with a reception with refreshments, wine, and live music being held from 5-7PM. We highly encourage all our artists to attend and to bring friends and family!
Learn more on UBC’s Arts in Medicine.
Hi! Hope you are well! I recently returned from the Virtual Medicine Conference at Cedars Sinai Hospital in Los Angeles. It was fantastic to learn from the diverse panel of researchers, physicians, and patients that are exploring other alternatives to treatment. A special hat tip to Surgeons and their Surgical Departments for their investment in technologies that assist in medical education, simulation training, and patient health. They’ve been such a positive and influential force in advancing care.
Although virtual reality is a new concept for many, the research in this area has been evolving for over 30 years. Virtual and augmented reality technologies are now contributing to prevention and wellness; objectives assessment and evaluation; functional training; improved interventions; facilitating adherence; and distributed care delivery. In medical training, VR/AR are being used for clinical, surgical, and interpersonal skills training; use of equipment and tools; team training in ER and Surgical departments; Emergency response training and rehearsal; and empathy. There’s a great deal of potential in these technologies and how they may help Canadians address our current healthcare challenges.
As it stands, Canada ranks 9th out of 11th in the Commonwealth Fund report. Canada ranks last in timely access to physicians and services and demonstrates an over reliance on expensive hospital care and on physicians. Canadians also rank lowest in access to their health information especially for people in rural and remote areas. Health records for Indigenous Peoples remain largely paper-based. Furthermore, there’s a lack of digital services for mental health issues. There’s a lack of coordination and fragmentation across the provincial and territorial health systems that’s also reflected in our siloed Electronic Health Record (EHR) infrastructure. Our EHR has yet to be tapped to improve our patient care.
How do we change this? By becoming aware and educated on these emerging technologies, exploring their use, and trying it out! If there’s a time to jump outside the box, it’s now!
I’ll be discussing the highlights and pearls gathered at the Faculty Development Breakfast on the 30th. For those unable to attend, here are a few resources and links that I gathered at this event and at the BC Health Summit (2018) for you to peruse:
Canadian Context
Intellectual, Behavioural, & Mental Health
Diagnosis, Assessment, & Recovery
Systems
Families & Children: Education & Health
Research, Articles, & Reports
Any questions or comments, please feel free to contact me or save them for the breakfast.
Warm regards!
Jacqueline

“We still talk in terms of conquest. We still haven’t become mature enough to think of ourselves as only a tiny part of a vast and incredible universe. Man’s attitude toward nature is today critically important simply because we have now acquired a fateful power to alter and destroy nature.
But man is a part of nature, and his war against nature is inevitably a war against himself. The rains have become an instrument to bring down from the atmosphere the deadly products of atomic explosions. Water, which is probably our most important natural resource, is now used and re-used with incredible recklessness.
Now, I truly believe, that we in this generation, must come to terms with nature, and I think we’re challenged as mankind has never been challenged before to prove our maturity and our mastery, not of nature, but of ourselves.”
Rachel Carson, Silent Spring (1963)
#EnvironmentalMedicine #SilentSpring
UBC researchers and companies founded by UBC faculty and students were recognized at the 21st Annual LifeSciences BC Awards on April 4.
UBC companies receiving awards:
Both Anandia and Aspect Biosystems received support from entrepreneurship@UBC, which provides the knowledge, tools and space for UBC entrepreneurs to succeed. Along with Terramera, Aspect also received funding from the UBC Seed Fund, which supports early stage UBC startups.
Creative Destruction Lab (CDL) – West, at UBC’s Sauder School of Business, won the Strategic LifeSciences Partner of the Year Award.
UBC researchers receiving awards:
Congratulations to all!
Barry Schwartz on Why We Work (2015)