Bright and early yesterday morning, I had the opportunity to facilitate an Academic Half Day (AHD) session with our UBC Family Practice Abbotsford-Mission residents on an increasingly important patient-safety issue: how to respond when ransomware or a major technology outage disrupts clinical care.
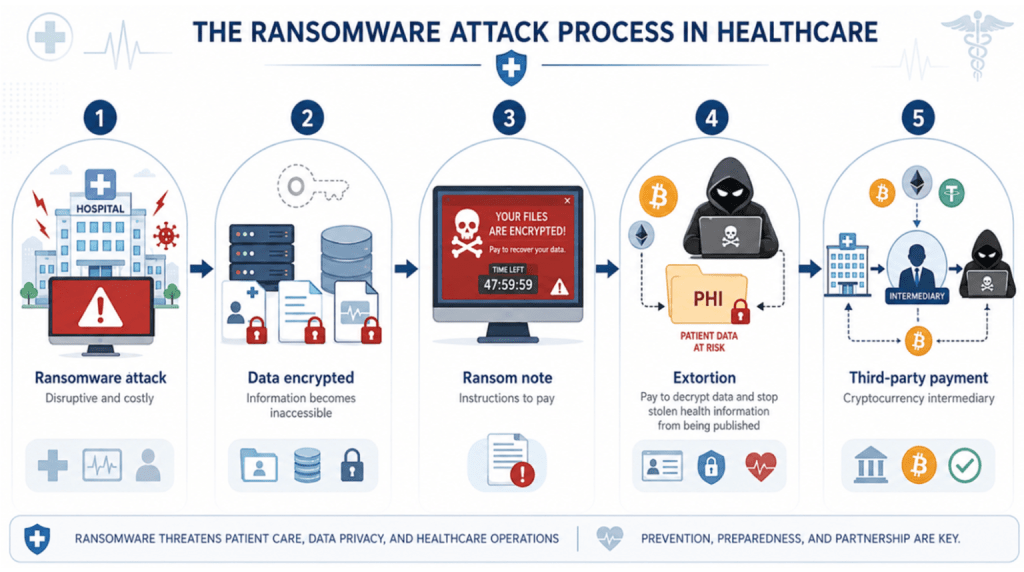
We began with a roundtable exercise exploring how residents would approach a ransomware attack: Who would they immediately contact? Which tasks would be essential? What tasks needed to transfer to paper, whiteboards, and face-to-face communication? And what were the greatest risks to patient care?
Then we dove into real-world examples, including the “WannaCry” ransomware attack and the CrowdStrike outage, and examined the impact that these two events had on healthcare systems, hospitals, clinicians, and patients. I also emphasized the important role our governments and healthcare systems play in tracking and reporting these incidents, conducting thorough debriefs, and disseminating findings and recommendations following these threat-to-life crimes.
To quote Black Widow in Spider-Man: Brand New Day, “This is big, big potatoes.”
If you just look at the Change Healthcare (UnitedHealth Group) ransomware attack in 2024:
* Records affected: 192,700,000
* Data exposed: names, addresses, dates of birth, Social Security numbers, government ID numbers, health insurance and policy numbers, etc.
* Aftermath: UnitedHealth reported roughly USD 3.1 billion in cyberattack-related impacts for full-year 2024, the most expensive healthcare cyber incident ever recorded. (https://www.upguard.com/blog/biggest-data-breaches-in-healthcare)
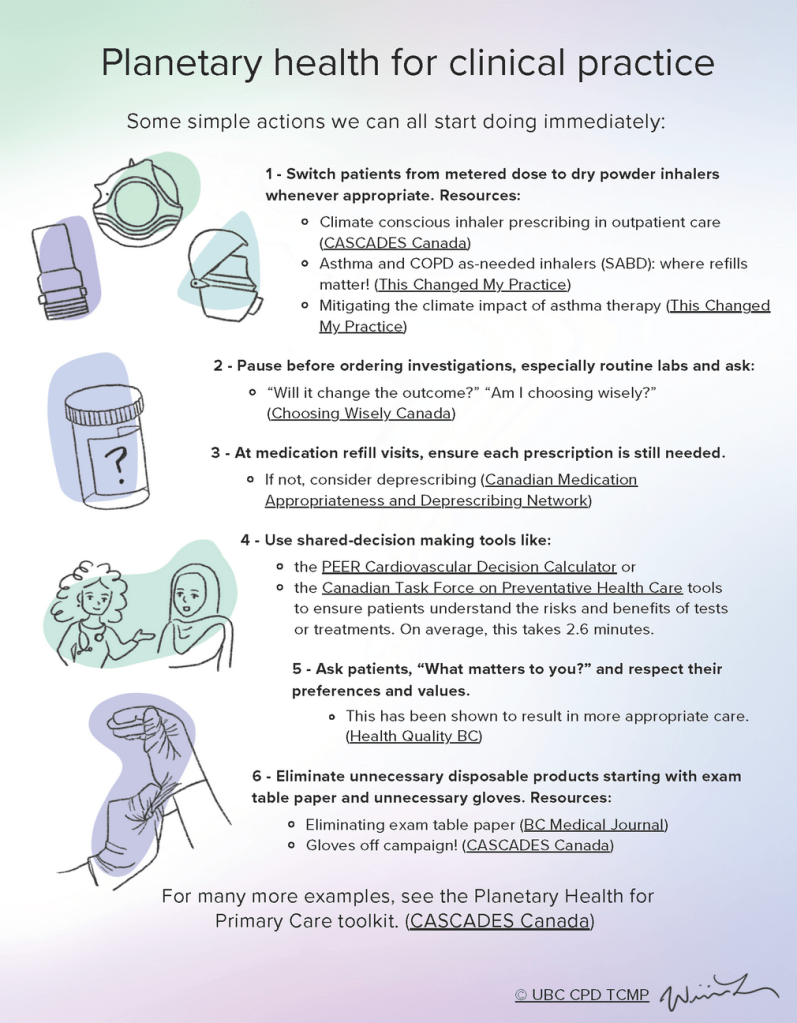
A key message from the session that I wanted to drive home was that we all have a role in cyber preparedness. Clinicians should be alert to any phishing attempts and clear on local downtime procedures, including knowing where approved paper resources are located, protecting patient information, and working closely with clinical, privacy, and technical teams during a disruption. These events also quickly highlight the importance in understanding how to work together as a team.
This is the first time “ransomware” has been addressed with our residents in the history of our site and I want to thank our Co-Site Director, Dr. Holden Chow, for allowing me the opportunity to facilitate this exercise.
To the residents reading this post, I encourage you to consider focusing a quality improvement project on educating and preparing your clinic for a ransomware attack or major technology outage. The time invested in strengthening your clinic’s preparedness could ultimately help save someone’s life.
#MedicalEducation#Cybersecurity#Ransomware#PatientSafety#HealthCare#ClinicalEducation#EmergencyPreparedness