On April 22, 1970, millions of people across the United States took to the streets to protest the negative impacts of 150 years of industrial development. Earth Day is now a global event each year, with more than 1 billion people in 192 countries taking part. Earth Day Network, the organization that leads Earth Day worldwide, has chosen the theme for 2019 of ‘Protect our Species‘.
Campaign goals
The Protect our Species campaign is designed to:
Educate and raise awareness about the accelerating rate of extinction of millions of species and the causes and consequences of this phenomenon.
Achieve major policy victories that protect broad groups of species as well as individual species and their habitats.
Build and activate a global movement that embraces nature and its values.
Encourage individual actions such as adopting plant-based diet and stopping pesticide and herbicide use.
How much do you know about the accelerating rate of extinction of millions of species and the causes and consequences of this phenomenon? Take the Earth Day quiz and find out.
“In British Columbia the current system of care for children with neurodevelopmental disorders does not appear to recognize there are two distinct patient populations: in one the children have few comorbidities and need limited specialized intervention and support, while in the other the children have significant mental health comorbidities and sometimes extremely challenging behaviors that require intervention for which funding is not readily available. Where this second population is concerned, vigorous family advocacy is required to access services and family breakdown can result. The Child and Youth with Special Needs division of the MCFD operates on an underlying assumption that parents are able and willing to take on a case manager role to access appropriate resources. This role is usually not appropriate for parents whose children have a dual diagnosis and require guidance and additional support to access specialized services.
BC needs policies and practices that recognize and address the complex needs of children with a dual diagnosis.”
Greetings Residents! Just a reminder that Journal Club is at my house this evening. And it’s sushi tonight…not Sofie’s Pizzeria :). Also, a reminder that Academic Half Day is tomorrow afternoon from 1330-1630. PIP projects are the focus so be prepared to update us all.
Are you a resident with an interesting story to share about surviving and thriving through training? Does your experience lend itself to a unique learning opportunity for fellow residents? If so, we want to hear from you!
International Conference on Residency Education (ICRE) 2019 planning committee is currently looking for participants to lead a practical discussion during this year’s Resident Survival Stories panel session, which will highlight both the challenges and triumphs experienced by residents.
The session will serve as an opportunity to share best practices and hear examples of successful navigation in the area of Diversity – Training in a world of differences: How it affects Residency Training
Deadline for submissions is May 20, 2019.
Candidates with stand-out stories will be invited to Ottawa to serve as panelists during the September 26-28 conference.
Join our UBC Abbotsford-Mission Family Practice Residency Program as we recognize our Residents’ scholarly achievements and celebrate our Preceptors who have contributed to our Residents’ journey! This informal evening is an opportunity for our Residents to share their research with our surrounding community and for our program to continue to network, collaborate, and build upon the ideas and insights emerging from our Residents’ work.
Date: Thursday, June 6, 2019 Location: Abbotsford Regional Hospital & Cancer Centre
Learning Centre Conference Rooms 3A & 3B
32900 Marshall Road, Abbotsford Time: Dinner (alcohol-free) begins at 7:00 p.m. / Presentations from 7:30 to 9:00 p.m. RSVP here!
Peruse the Agenda & Scholar Project Summaries here. If you have any questions, please feel free to contact me at jacqueline.ashby@ubc.ca.
Meet Dr. Leslie Meloche! She works as a family doctor in Abbotsford and is one of the 1500+ valued preceptors across the province who dedicate time, energy, and thought to supporting UBC Family Practice residents. She’s also a graduate of the UBC Abbotsford-Mission Family Practice Residency program! This week she shares with us her insights on teaching and learning as one of our new community preceptors.
Who do you teach?
I currently “teach” one family practice resident. This is my first year being a co-preceptor for the family practice residents. As I am fairly new to practice, I had little experience with teaching residents or medical students in the past. I emphasize “teach” as that implies that I am the only one imparting knowledge. However, I feel that most days teaching is reciprocal and occurs on many more levels than just preceptor to resident. I am constantly learning as well, not only from the residents, but also from my patients, colleagues, staff and my family.
What inspired you to teach?
Honestly, I had not yet reached a point in my medicine career where I felt inspired to teach (probably because I felt I was still learning and had little wisdom to share with others). I was given a gentle nudge to become a preceptor in the program.
Who was the educator that had the most impact on you and why?
I have had so many great educators that it is hard to name just one. But I do remember a rural family doc in Alberta that I encountered in medical school. He was so excited about family medicine. He would share cases of all the interesting pathology that he would see, but then put it in the context of the patient’s life. You could tell he really valued the relationships he had with his patients and how much more interesting his work was because of this. I think this really highlighted the reason I chose family medicine as a career over other specialties.
As a new preceptor, what’s your best piece of advice to those making the transition from practice to preceptorship?
Just do it and don’t be afraid. You actually do have wisdom and experience to share, despite what you might think.
If you could change one thing in our healthcare system overnight, what would it be and why?
A universal provincial electronic medical! So that we could all communicate effectively with one another to improve efficiency and provide better care.
Vulnerability is hard, and it’s scary
And it feels dangerous
But it’s not as hard
Scary or dangerous
As getting to the end of our lives
And having to ask ourselves
What if I would’ve shown up?
“Many of the people I admire lead lives that have a two-mountain shape.
…
If the first mountain is about building up the ego and defining the self, the second is about shedding the ego and dissolving the self. If the first mountain is about acquisition, the second mountain is about contribution.
…
Over the past few decades the individual, the self, has been at the center. The second-mountain people are leading us toward a culture that puts relationships at the center. They ask us to measure our lives by the quality of our attachments, to see that life is a qualitative endeavor, not a quantitative one. They ask us to see others at their full depths, and not just as a stereotype, and to have the courage to lead with vulnerability. These second-mountain people are leading us into a new culture. Culture change happens when a small group of people find a better way to live and the rest of us copy them. These second-mountain people have found it.”
More on The Moral Peril of Meritocracy: Our Individualistic Culture Inflames the Ego and Numbs the Spirit. Failure Teaches Us Who We Are. By David Brooks via The New York Times. (Thank you Tina for sharing!)
Greetings! Our Department of Family Practice is currently exploring the clinical placement model and environment. Given this, our Abbotsford-Mission site took the opportunity to use the design thinking process to consider how the clinical learning setting would look if it were to:
1. Support the inclusion and practice of medical students, residents, clinical educators, and their staff, and;
2. Offer patients interdisciplinary, team-based care.
During our Academic Half Day, we assembled in teams of 2-3 and went through a series of steps including:
1. Create a Blueprint: Plan and draw out the space. Describe the objectives of each area and services provided.
2. Design a Narrative: Describe the experience and transition of patients, learners, and educators within the environment.
3. Illustrate the Accommodation: Describe the activities, resources, and number of users that may be accommodated.
Here are the results of our three teams:
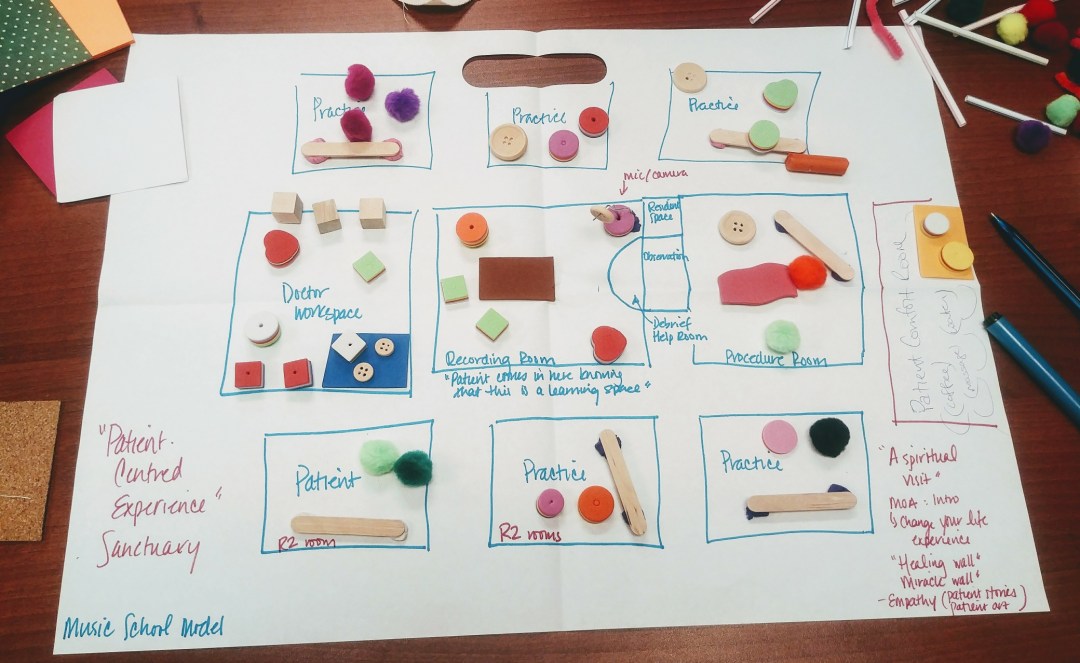
TEAM ONE: Patient-Centred Sanctuary: Music School Model
Patient-Centred Sanctuary: Music School Model
A music school is the inspiration behind the physical design and layout of the space. The clinic’s objectives include offering patients a sanctuary that is safe and comforting in addition to providing learners an environment that is centred on education and patient inclusion. The patient enters the space on the right side and is greeted by the medical office assistant (yellow rectangle).
The patient area is surrounded by “empathy” and “healing” walls. The “Empathy Wall” contains patient stories and art. In this room they are offered services such as coffee, water, massage, and aromatherapy. In the middle of the space is the “Recording Room” (brown rectangle) where the student and/or resident, preceptor, and patient explore learning. Patients invited into the Recording Room are intimately involved in the learning process and assist both preceptor and learner in delivering care. There is an “Observation Room” directly attached to the right of the Recording Room for learners, educators, and patients to observe, provide constructive feedback, and debrief.
Above the Observation Room is a small private “Resident/Student Space” designated for computer work, note taking, etc. To the right is a large “Procedure Room” (pink rectangle) that allows for the team to watch and engage with both spaces. To the left of the Recording Room is the “Doctor Workspace” (blue rectangle) that offers an open concept setting allowing for physicians to converse on patient, teaching, and learning matters. Surrounding the Recording Room are a series of “Practice Rooms” designed for R2s who require less observation in their work with patients and more hands-on experience.
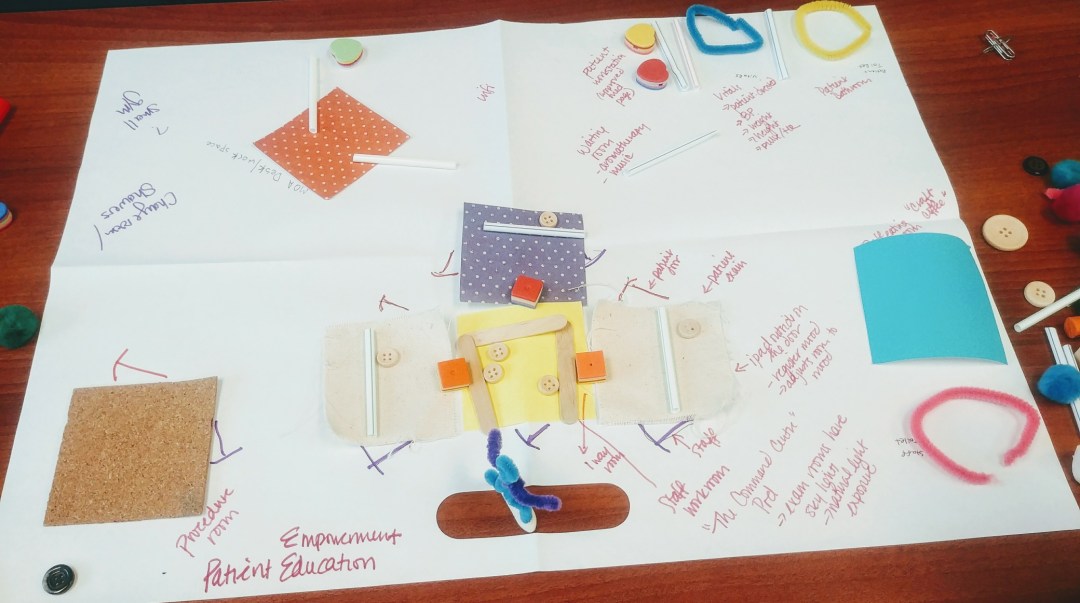
TEAM TWO: Patient Education & Empowerment Model
Patient Education & Empowerment Model
The objectives of this clinic include empowering and educating patients as well as supporting physician wellness and learning. Patients arrive at the top centre of the layout where they are greeted by the medical office assistant (represented by orange polka-dot square). As the patient enters the space, they experience aromatherapy and light music.
To the right of the room, there are a series of “Patient Workstations” (heart-shaped cushions) and wifi that offer access to patient-centred educational websites and resources. Once greeted and checked in, the patients are then asked to head into the room on the right that educates them on taking their own vitals including blood pressure, heart rate, weight, and height. Next to the “Vitals Room” (blue pipe cleaner) there is a “Patient-Dedicated Bathroom” (yellow pipe cleaner) to the right of this space.
In the centre of the office is the ”Learning/Command Centre Pod” (yellow, white, purple polkadot squares) that has a series of “Patient Exam Rooms” (white squares) where students, residents, and preceptors meet with clients. As patients enter the room, they come upon an iPad located at the door that registers their mood and responds by adjusting the exam room’s lighting, scent, and music to provide greater patient comfort. Each room is outfitted with one door for staff and one door for patients as well as a skylight for natural light.
The “Staff Workroom” (yellow square) is where physicians and learners can convene to discuss their experiences. There are one-way mirrors that connect the Staff Workroom to the surrounding patient rooms allowing for observation. To the right of the Learning Pod, is the dedicated “Staff Bathroom” (pink pipe cleaner) and “Meeting Room” (blue square) serving treats and craft coffee. To the left of the Learning Pod is the “Procedure Room” (cork square) again offering two separate doors for staff and patients. In the top left-hand corner, there is the “Staff Gym” and “Change/Shower Room” that encourage employee health and wellness.
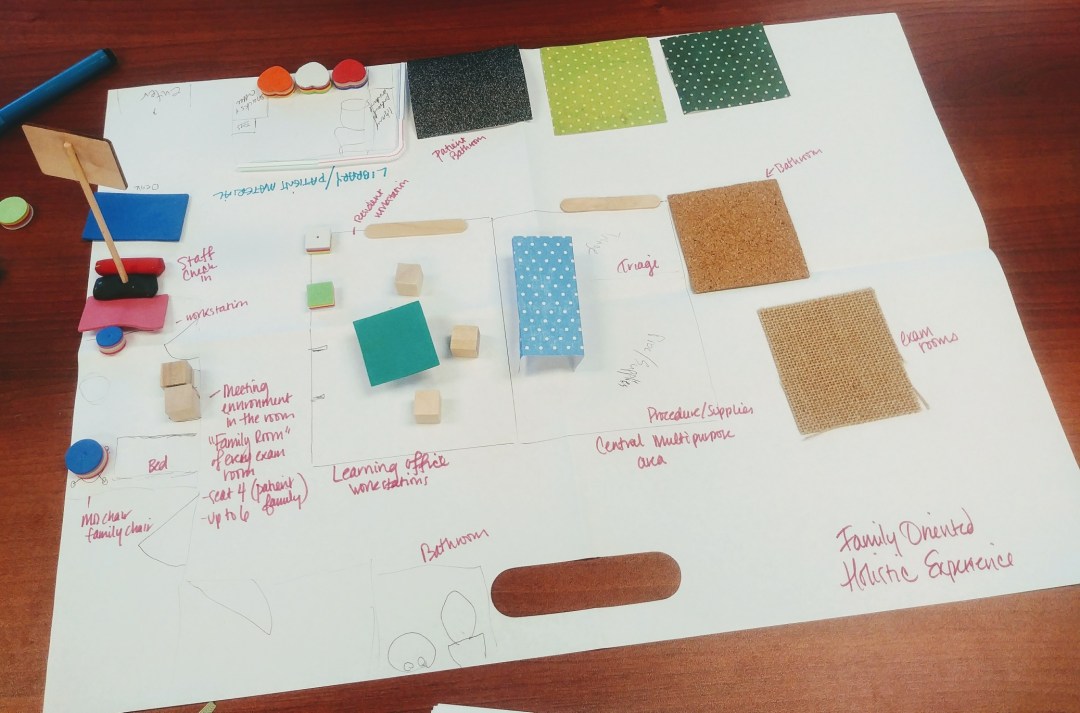
TEAM THREE: Patient-Family Oriented Model
Patient-Family Oriented Model
The main objectives of this clinic include creating an inviting and inclusive environment for the patient and the patient’s family members. The residents working on this space discussed the increasing presence of family members at their clinics and felt the need to accommodate them.
The patient enters the setting from the top left-hand corner (blue rectangle) and is greeted by a medical office assistant at the front. On the right side, they have access to comfortable seating (heart-shaped cushions), a library, snacks, coffee, and toys for the kids. To the right of the “Patient Learning” area is the “Patient Bathroom” (black square). On the far left, the patient enters the exam room, now identified as the ”Family Room” (pink rectangle) where patients and their family are encouraged to make themselves at home. These rooms are fairly large in that they can accommodate for up to 4-6 people.
In the centre of the space is the “Learning Office” (aquamarine square) outfitted with a series of “Workstations“. To the right of that room is the “Procedure/Supplies Room” (light blue polkadot rectangle) empowering and educating both learners and the patients on the procedures being performed. Surrounding the space are varied “Exam Rooms” for learners and educators to see patients and debrief their experiences.
In summary, this exercise emphasized that there are several ways to think about a clinical learning space that is designed to address a variety of patients’ needs while also accommodating for one’s learning and development. All the models illuminate the creativity and genius of our Residents as they take their experiences and ideas and articulate them on paper. I hope this provides others the inspiration to tinker with their clinical space and consider other alternatives and perspectives as to how people experience their environment.
A big thank you to our Residents for participating and providing your insights and thoughts on how we can design a clinical learning environment for the present and future of healthcare.


 Cue the Jeopardy
Cue the Jeopardy 
 Meet Dr. Leslie Meloche! She works as a family doctor in Abbotsford and is one of the 1500+ valued preceptors across the province who dedicate time, energy, and thought to supporting UBC Family Practice residents. She’s also a graduate of the UBC Abbotsford-Mission Family Practice Residency program! This week she shares with us her insights on teaching and learning as one of our new community preceptors.
Meet Dr. Leslie Meloche! She works as a family doctor in Abbotsford and is one of the 1500+ valued preceptors across the province who dedicate time, energy, and thought to supporting UBC Family Practice residents. She’s also a graduate of the UBC Abbotsford-Mission Family Practice Residency program! This week she shares with us her insights on teaching and learning as one of our new community preceptors. “Many of the people I admire lead lives that have a two-mountain shape.
“Many of the people I admire lead lives that have a two-mountain shape.