With summer right around the bend here’s an image of 69-year-old man with unilateral dermatoheliosis caused by ultraviolet rays that had penetrated the window glass of his delivery truck that he drove for 28 years. “Chronic UVA exposure can result in thickening of the epidermis and stratum corneum, as well as destruction of elastic fibers. This photoaging effect of UVA is contrasted with photocarcinogenesis.”
Read more on Unilateral Dermatoheliosis by Jennifer R.S. Gordon, M.D. & Joaquin C. Brieva, M.D. via The New England Journal of Medicine
Vancouver, British Columbia (2019). Image via J. Ashby
“We may sometimes feel that we can’t do much as individuals, but humanity is made up of individuals; we can make a difference. As individuals we can influence our own families. Our families can influence our communities and our communities can influence our nations.”
Dylan Goode, a graduate researcher at Heart Valve Performance Laboratory at UBC Okanagan’s school of engineering, holds one of the new heart valves. UBC
Congratulations to UBC Okanagan researchers who have made a breakthrough in making heart surgery safer and less invasive by creating a synthetic heart valve! Read more here about their recent discovery.
#UBCO
“In order for the promise of digital health to be realized, companies will need to ensure their patients’ data is safe, secure and error-free. Beyond security, healthcare companies operating as providers must also maintain the confidentiality and privacy of that data. Doing so isn’t simply good practice; it’s an existential requirement for companies operating in this space. There is a baseline expectation — from users, and from employers and health plans working with digital health companies — of privacy being maintained.”
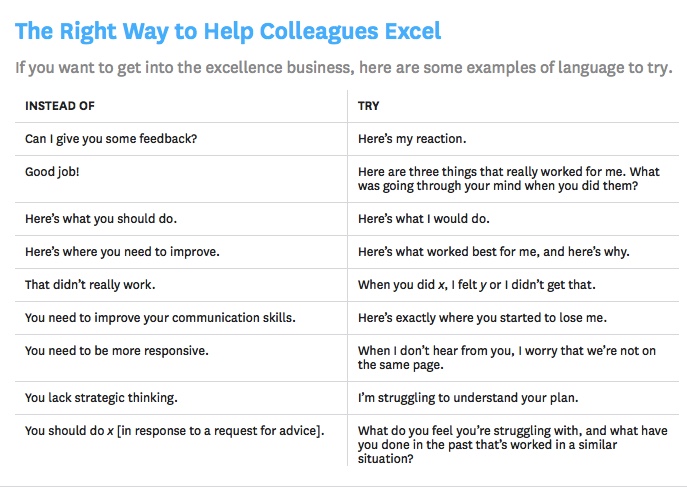
“We humans do not do well when someone whose intentions are unclear tells us where we stand, how good we ‘really’ are, and what we must do to fix ourselves. We excel only when people who know us and care about us tell us what they experience and what they feel, and in particular when they see something within us that really works.”
More on The Feedback Fallacy (March-April 2019) by Marcus Buckingham & Ashley Goodall via Harvard Business Review.
“The guideline, which is structured using a clinical reasoning pathway, includes 11 evidence-based recommendations and, where clear evidence is not available, 19 consensus-based recommendations. The guideline provides tools to assist assessment and diagnosis, and includes recommendations on the work-relatedness of mental health conditions, patient management including decisions about return to work, comorbid or secondary mental health conditions, conveying a diagnosis to a patient and communication with others in the workplace. It promotes collaboration, communication, cultural sensitivity and appropriate care, highlighting the important role that can be played by family physicians, and the members of their teams, in each person’s personal recovery and return to work.”
The next International Association for Medical Education (AMEE) webinar hosted by the AMEE Simulation Committee will be presented by Walter Eppich – “Learning through talk: exploring synergies between simulation and workplace learning” on Friday 29th of March at 2:00 pm (GMT/UK) / 7:00 a.m. (PST) .
Talk as joint social activity impacts communication practices, learning, and patient care. This session will explore the important role of talk in both simulation and workplace settings.
Lessons learned from healthcare debriefing will help us identify ways to address the ‘process’ and ‘content’ of talk of clinical practice to promote learning and patient care.
As of 2019, the AMEE webinar series will be entirely free you can access the webinars by joining here when the webinar begins.
Due to limited space it is advisable to join on time as AMEE cannot guarantee entry to webinars.
Greetings! This week I’m headed down to the Virtual Medicine Conference at Cedars-Sinai Hospital in Los Angeles. I recently learned that organizers will livestream the event for free. This means you can join me! Access the conference agenda and livestream here. Conference starts on Wednesday, March 27 at 9:00 a.m. Hope to catch you there!
Emergency physicians are frequent providers of Indigenous health. Emerging evidence suggest implicit bias to be a contributor to health disparities affecting Indigenous Canadians. This presentation explores the impact of implicit bias as well as strategies to mitigate its adverse effects in the Emergency Department.
A big thank you to our former UBC Abbotsford-Mission Family Medicine resident, Dr. James Liu, for posting your presentation and sharing your work! And thank you to Dr. John Pawlovich for forwarding the link!
Jeff Kornelsen works as a family doctor in Mission and is one of the 1500+ valued preceptors across the province who dedicate time, energy, and thought to supporting UBC Family Practice residents. What keeps Dr. Kornelsen inspired?
Who do you teach?
Anyone who will listen! I would teach my kids more but they’re adults now and are sometimes less inclined to listen…actually I have learned that it’s not much good to teach all the time. I do enjoy teaching residents, colleagues, and coworkers, and most of all I teach patients, all day, every day at work.
What inspired you to teach?
My profession has taught me a lot. I think, like most people who have a fair bit of experience, I have something to give. Teaching one patient can make a big difference to that person but teaching a resident could have generations of impact!
Who is one educator that had a significant impact on you? What did s/he do that was so effective?
My dad was a teacher. I think I caught his passion for teaching. Dr. Ed Korchinski was my favorite preceptor. Nothing phased him. He was always steady, wise, and supportive.
How do you establish and maintain a good working relationship with your resident?
Definitely the most important thing is to be interested in who they are. Respecting them should follow naturally. Of course you will uncover learning needs, but find out what their felt needs are, and address those.
What do you predict will be our biggest medical advancement in the year 3000?
I have no idea what that year will entail! But long before then, we will be treating conditions genetically. I’m pretty sure most traces of today’s medicine will be unrecognizable. Somehow patients will still need to be known and cared for; I don’t think you can have genuine movement toward health without that.