

BC Women’s Hospital Research Rounds

“While most companies run employee-recognition programs of some sort, all too often they produce reactions like Rowen’s. Instead of giving people a meaningful sense of appreciation, they become just another box for managers to check and are completely disconnected from employees’ accomplishments. Some companies try to make programs more relevant by giving specific awards to individuals who’ve, say, created and led an important new initiative, “embodied” the organization’s values in their behavior, or had a significant impact. Yet that approach has problems too: Awards can be seen as an elite opportunity for a chosen few — and leave the majority of the workforce feeling left out and overlooked.
If managers could make a far broader group of employees feel appreciated, the benefits would be considerable. Adam Grant and Francesca Gino have found that when people experience gratitude from their manager, they’re more productive. Another researcher recently found that teams perform tasks better when their members believe that their colleagues respect and appreciate them.
But in our combined 50-plus years of working to improve organizations, we’ve observed that many managers struggle to make employees feel that their talents and contributions are noticed and valued. To explore this problem, we recently took a deep dive within an organization to see how organizational efforts to show appreciation and gratitude were perceived. In that project we engaged with both employees and managers through focus groups, survey questions, and learning sessions. And what we discovered was that even though bosses feel it’s challenging to show their staff appreciation, the employees think it’s actually pretty simple.”
More on The Little Things That Make Employees Feel Appreciated via Harvard Business Review.
“Health care professionals and systems have an essential role in comprehensive strategies to reduce violence and suicide and corresponding inequities in communities. However, medical school curricula do not consistently incorporate firearm safety, violence prevention, or social determinants of health in training. Many clinicians are not comfortable asking patients about firearm injury risk factors2 and are not trained in trauma-informed care. At the health system level, financial incentives prioritize rapid visits and higher volume that leave less time for patient counseling and prevention; yet the financial costs to systems from caring for individuals who experience firearm-related trauma is substantial.
Many clinicians may not have the experience or be aware of the opportunities to prevent firearm-related morbidity and mortality. For example, in a survey of 1015 family physicians, 46% reported no training in firearm safety counseling and 68% did not feel knowledgeable discussing safe storage devices for firearms. Family physicians who had received formal training about firearm safety counseling were more likely to report a higher level of comfort with asking patients about firearm ownership.3 Physicians and other health care professionals can enhance the safety of their patients, improve data to inform community efforts, and support system changes to prevent violence and reduce inequities. Examples include pediatricians asking parents about safe storage of firearms at home, emergency physicians and surgeons engaging in hospital-based violence intervention programs and referring injured patients to wraparound services (such as counseling and job training), and behavioral health practitioners assessing suicidality and counseling about access to lethal means. Clinicians also can work with health departments and community partners to share their medical and health care–related expertise in regard to policies and programs that increase economic and household stability and enhance access to care, services, and support (e.g., tax credits, housing policies, mentoring, and after-school programs).4“
More on Firearm Homicide and Suicide During the COVID-19 Pandemic Implications for Clinicians and Health Care Systems via JAMA.
ABSTRACT: Outpatient parenteral antimicrobial therapy is an important medical service that allows for the treatment of complex infections outside acute care hospitals. In BC, the practice has evolved over many decades to include both hospital-based and outpatient infusion centres, as well as home intravenous programs. Numerous publications demonstrate the safety, efficacy, and cost reduction of outpatient parenteral antimicrobial therapy, while reducing congestion in emergency departments. With increasing strain on inpatient facilities due to increased numbers of drug-resistant organisms and high-risk immunosuppressed patients with complex infections, outpatient parenteral antimicrobial therapy is a treatment modality that improves patient care and flow through the health care system.
More on Delivery models, efficacy, safety, and cost reduction of outpatient parenteral antimicrobial therapy in British Columbia via BCMJ.
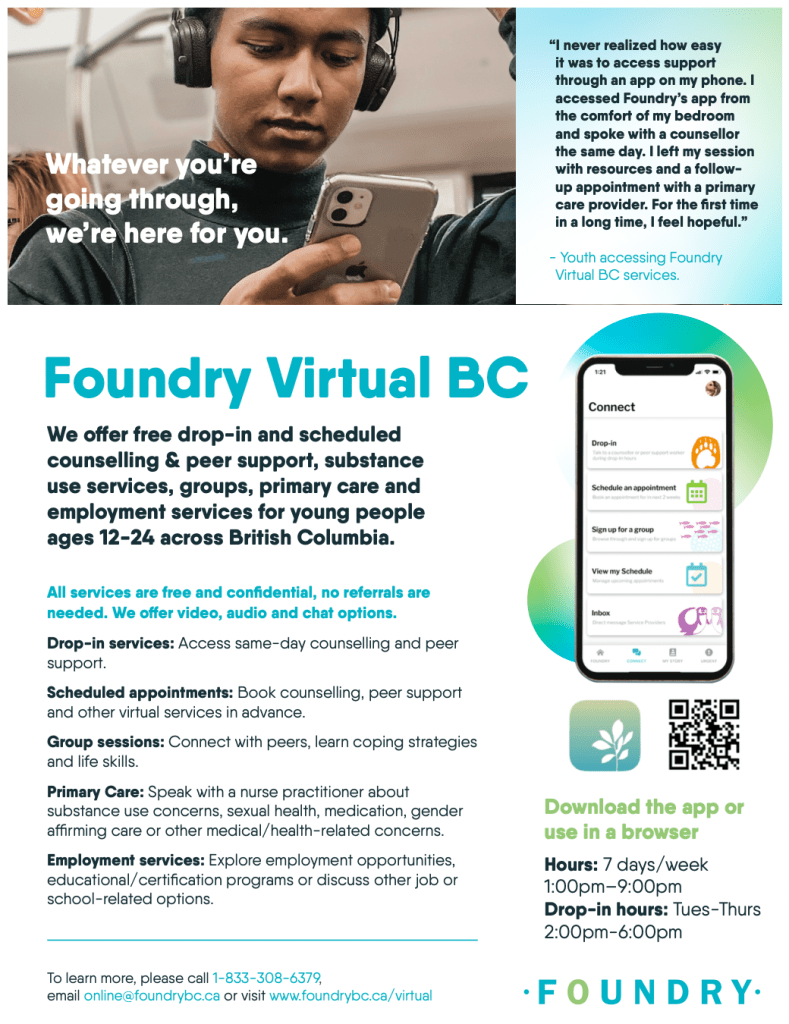
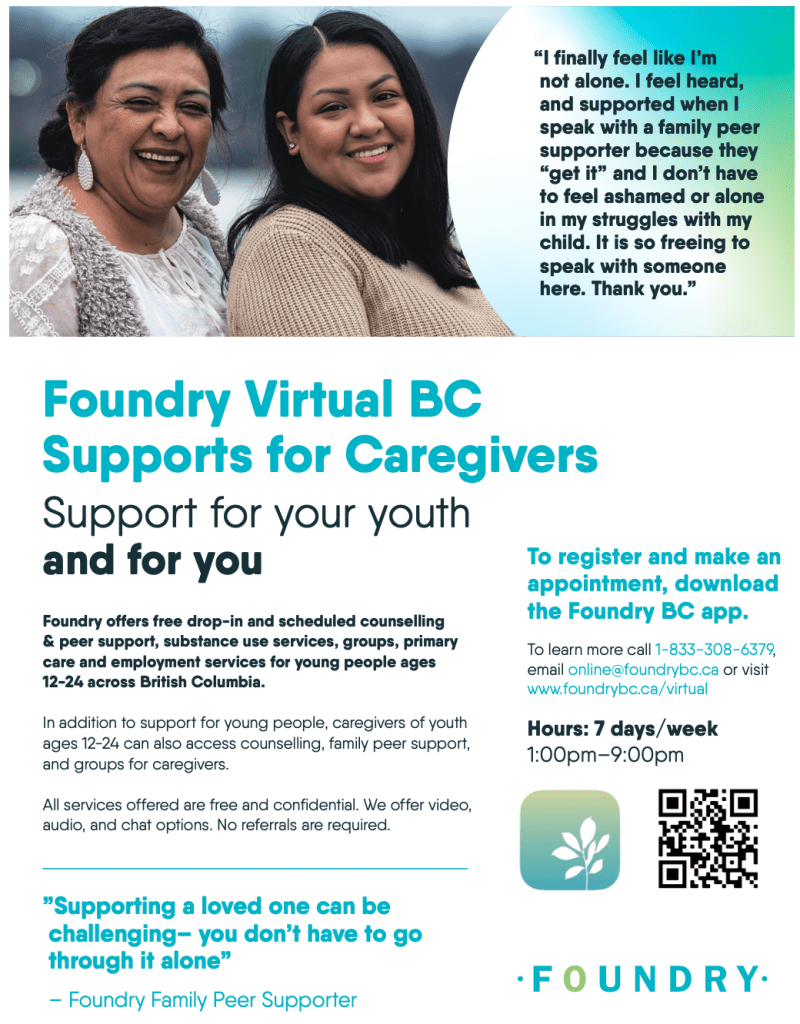
Foundry Virtual BC offers free services for youth ages 12-24 and their caregivers anywhere across BC. Services offered includecounselling & peer support, substance use services, groups, primary care, employment services, and Indigenous wellness services. Foundry currently has 11 centres open across the province which you can see here with 8 more centres opening in the next couple years. Foundry Virtual BC’s goal is to support communities across the province that do not have a Foundry centre, specifically rural and remote communities, by downloading the Foundry BC app (this can also be accessed on our website portal) which offers video, audio and chat options.
KEY POINTS
“Infection with high-risk strains of the human papillomavirus (HPV) is a known prerequisite for developing cervical cancer. Soon, a test for high-risk strains of HPV will replace the Papanicolaou (Pap) test for routine cervical cancer screening in Canada. Unlike the Pap test, which requires a cytopathologist to detect precancerous cervical cells, testing of a cervical sample for HPV subtypes uses polymerase chain reaction (PCR). Australia, the Netherlands and the United Kingdom have adopted the HPV testing model for cervical screening, and it is also endorsed by the American Cancer Society. A recent review by the Canadian Agency for Drugs and Technologies in Health considered available evidence; its report concluded that HPV PCR testing of cervical samples is better at detecting precancer or cancer than Pap testing and would decrease the overall cost of screening. However, shifting to this new screening modality will mean overhauling existing algorithms for age and screening intervals, changing resource allocation and educating physicians and patients. We discuss why and how cervical screening will need to change in Canada with the adoption of the new test.”
Shifting from cytology to HPV testing for cervical cancer screening in Canada via CMAJ.
More on the Human Papillomavirus vaccine via ImmunizeBC.
“Both Whitmer and Planned Parenthood have sued to overturn Act 328. But their arguments depend heavily on rulings the Supreme Court now appears ready to reverse: Roe v. Wade and Planned Parenthood v. Casey.
Michigan residents seeking abortions will likely turn first to Illinois — but for a woman in Detroit, Windsor could be closer. The average cost of an abortion in Canada is also slightly lower than in many U.S. states.
Robert Currie is an expert on transnational criminal law at Dalhousie University in Halifax.
‘I think there’s certainly a possibility that people will cross the border into Canada,’ he said, ‘either to avoid criminal prosecution for having obtained an abortion or to be able to obtain one. In either situation, there’s the potential for it to create an international incident of some kind.'”
More on Roe v. Wade is on the brink — and Canada could be pulled into U.S. brawls over abortion law via CBC.

“Skill is the child of patience.”~ Obi-Wan Kenobi
#MayThe4thBeWithYou

“This was a qualitative study utilizing a phenomenological approach. The purpose was to determine what rehabilitation strategies physical therapists use with dancers and to discuss techniques for implementing these strategies from both the dancer’s and the physical therapist’s perspectives. Self-administered questionnaires were sent via email to dancers and physical therapists. Purposeful sampling was done through use of a criterion sampling method that required participants to have experienced dancer rehabilitation. Data were correlated to find common strategies and to encourage modification of current approaches. Physical therapists returned 29 surveys, while dancers returned eight. Five themes were identified in the areas of: 1. evaluation, 2. dance modification, 3. interventions, 4. education, and 5. communication. The conclusion of this study was that successful rehabilitative strategies involve ongoing evaluation that incorporates knowledge of dance technique and performance, dance-centered movement modification that is clearly defined, and an understanding of dance lingo.”
Read more on Physical therapy rehabilitation strategies for dancers: a qualitative study via J Dance Med Sci.
