Dr. Bob Bluman of UBC’s CPD and Toby Achtman, Executive Director of BCCFP, have created a series of helpful videos on diagnosing patients virtually. Please see below to learn more:
“Radiation has been a staple of cancer treatment for decades, with approximately 50 per cent of cancer patients receiving radiation therapy at some point in their journey.
While effective, traditional radiation therapies rely on intense beams of energy shot from outside the body. These beams can kill cancer cells, but their use is limited to select locations, making them less suited for difficult-to-treat metastatic cancers that have spread to multiple sites.
Now, a UBC-led team of Canadian researchers has received $23.7 million in federal funding to develop a new generation of radiation therapy, known as radiopharmaceutical therapy, that delivers highly targeted doses of radiation from within.”
Learn more on “Nuclear medicine can cure cancer, and Canadian researchers are stepping up the fight” via UBC’s Faculty of Medicine.
On behalf of the UBC FP Residency Program, we would like to congratulate our residents on receiving several 2023 BCCFP awards as announced by the BC College of Family Physicians yesterday!
Rachel Cook: R2 Resident Award Robin Craven: R2 Resident Award Cassia Tremblay: R2 Resident Award Arielle Roberts: Dr. Manoo and Jean Gurjar Award Nique Seper: Dr. Manoo and Jean Gurjar Award
Please join us in celebrating our residents’ achievements! You can read more on these (and other, such as BC Physician of the Year) awards here.
Jana Ogdenova Senior Co-Manager, Faculty of Medicine Department of Family Practice, Postgraduate Program
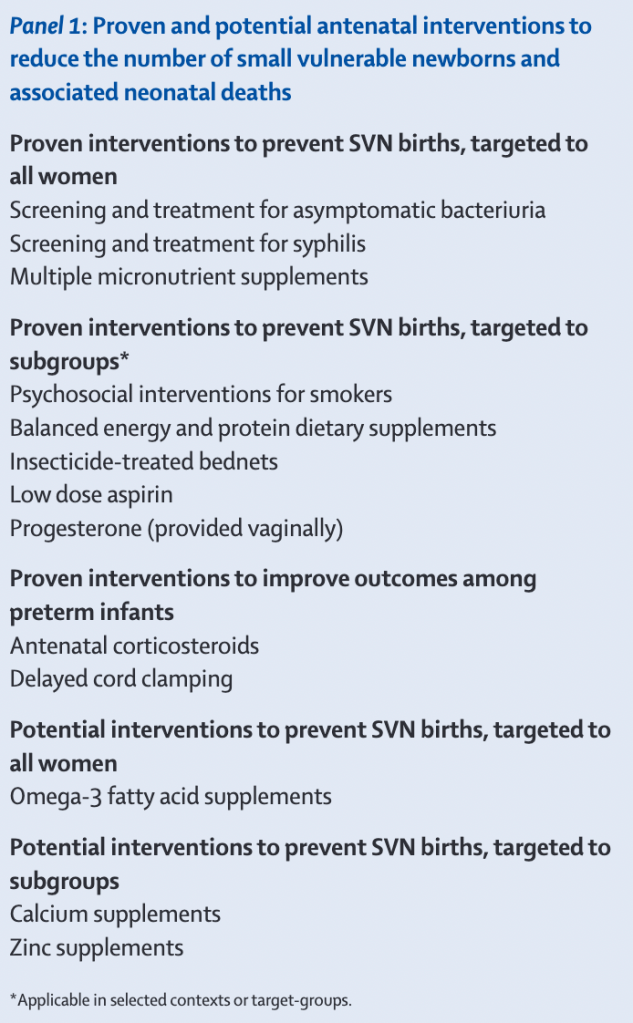
“The fact that every fourth baby in the world is born too soon or born too small is a concern for human rights, public health the national economy, and development. By not addressing this priority, we are jeopardising our collective future.”
The lives of more than a million babies a year could be saved across the developing world if mothers were given access to simple, low-cost health measures such as vitamins, antimalarials and aspirin, a new analysis has found.
The study, focused on the “silent public health disaster” of babies being born “too small or too soon”, comes as the United Nations warns that progress on reducing newborn deaths and stillbirths has flatlined since 2015, and that patchy, underfunded antenatal care is partially to blame.
The authors of the analysis, published in the Lancet, estimate that 476,000 newborn deaths and 566,000 stillbirths could be avoided every year if a handful of predominantly antenatal measures were fully implemented in 81 low- and middle-income countries.
Learn more on Small Vulnerable Newborns via The Lancet.
Background: We explored health care services in three supportive housing sites in Kelowna, British Columbia, to identify tenants’ health needs and determine whether their needs were perceived as being met, and, if their needs were perceived as not being met, which health areas were being underserved.
Methods: We invited all tenants and staff at the supportive housing sites to provide information on their health needs and related support. In-depth interviews were conducted between 1 August and 2 September 2020, including both closed-ended and open-ended questions.
Results: In total, 42 tenants (38%) and 30 staff members (75%) were interviewed. Seventy-two percent of tenants interviewed had unmet health needs; those with developmental disabilities experienced the highest percentage of unmet needs. Long-term conditions such as diabetes, high blood pressure, heart disease, and liver disease were also associated with unmet needs. Tenants were often unaware of available health care services or were unwilling or unable to access them. Both tenants and staff emphasized that stigma and discrimination within health services are a barrier to receiving care. Existing health services were also seen as ill-equipped to deal with concurrent conditions, such as mental health issues, substance use, and/or physical disability.
Conclusions: We recommend that further research be conducted on the needs of other populations in supportive housing across BC and that additional funding be provided to create a wide range of housing options to address the diverse health, social, and other needs of tenants.
Read more on Health care in supportive housing facilities via BCMJ.
May 5 marks the National Day of Awareness for Missing and Murdered Indigenous Women, Girls and Two-Spirit people (MMIWG2S) in Canada, also known as Red Dress Day. The day is about building awareness and honouring those who were lost and their families.
Remembering and acknowledging the injustices, the lack of follow-up, the lack of resolution. These families have lived with this for years, and in some cases for decades. And so having a Red Dress Day, and recognizing that these stories occur. That these families are still looking for answers, and that this can’t continue to happen. That is what we are doing today: trying to address a wrong that has taken place for many years and many decades.
As Canadians commemorate Red Dress Day in Canada, local government leaders are keen on addressing the national inquiry on Missing and Murdered Indigenous Women and Girls (MMIWG) and the report’s 231 Calls for Justice.
Indigenous women and girls are five times more likely to experience violence than any other population in Canada, and Indigenous women make up 16 per cent of all female homicide victims and 11 per cent of missing women, despite representing just 4.3 per cent of the population, the organization says.
For many years, government policy in regards to Indigenous people has been more reactive than preventative, and policy with regards to missing and murdered Indigenous women and girls (MMING) is no exception.
Imagine that your daughter or sister or mother disappeared – and when you asked for help from police, your concerns weren’t taken seriously. Then, a week later her body is discovered. While the exact details of the story may vary, this is the current scenario for thousands of family members of missing and murdered Indigenous women. After years of advocacy and emotional turmoil, a national inquiry has finally been struck to find out what went wrong and how to fix it.
Question Can an artificial intelligence chatbot assistant, provide responses to patient questions that are of comparable quality and empathy to those written by physicians?
Findings In this cross-sectional study of 195 randomly drawn patient questions from a social media forum, a team of licensed health care professionals compared physician’s and chatbot’s responses to patient’s questions asked publicly on a public social media forum. The chatbot responses were preferred over physician responses and rated significantly higher for both quality and empathy.
Meaning These results suggest that artificial intelligence assistants may be able to aid in drafting responses to patient questions.
Learn more on Comparing Physician and Artificial Intelligence Chatbot Responses to Patient Questions Posted to a Public Social Media Forum via JAMA.
“Deep generative networks in recent years have reinforced the need for caution while consuming various modalities of digital information. One avenue of deepfake creation is aligned with injection and removal of tumors from medical scans. Failure to detect medical deepfakes can lead to large setbacks on hospital resources or even loss of life. This paper attempts to address the detection of such attacks with a structured case study. Specifically, we evaluate eight different machine learning algorithms, which include three conventional machine learning methods (Support Vector Machine, Random Forest, Decision Tree) and five deep learning models (DenseNet121, DenseNet201, ResNet50, ResNet101, VGG19) in distinguishing between tampered and untampered images. For deep learning models, the five models are used for feature extraction, then each pre-trained model is fine-tuned. The findings of this work show near perfect accuracy in detecting instances of tumor injections and removals.”
Myles Sergeant, a family physician in Hamilton, Ont., launched one such effort to cultivate partnerships on climate action across healthcare facilities, called PEACH.
He was inspired by a paper published in TheLancet Planetary Health which showed that more than 60% of the emissions generated by England’s National Health Service were related to the supply chain, rather than the delivery of care (24%), or travel by staff, patients, and visitors (10%).
Looking further into the issue, PEACH developed a checklist of the 20 most impactful actions hospitals could take to reduce their carbon footprint – in some cases, at low cost or savings. These include divesting foundation funds from fossil fuels, implementing Choosing Wisely programs to reduce waste, using reusable gowns and linens, adopting sustainable prescribing strategies, increasing plant-based food options for patients, and weighing sustainability in procurement contracts.”
How Canadian hospitals are decreasing carbon emissions via CMAJ.