Thank you for the steady presence you bring to every clinic day, and for the care you deliver when the work is complex and the pace is relentless. Thank you for showing up with curiosity, humility, and courage, for asking the hard questions, and for learning in real time with patients and teams who rely on you. You carry responsibility with grace, you make space for compassion in the middle of urgency, and you keep aiming to do better, even when you are tired.
Resident Doctors Appreciation Week is a small pause in a very busy year, but the gratitude is real. We see your effort, we value your growth, and we are proud to support you as you become the physicians our communities need.
Assessment works best when we share the same mental model. Ahead of our March 2 retreat, we are using a short quiz to refresh key points from the CFPC resident assessment standards and to identify where we need clearer alignment across sites.
The goal is practical: reduce friction for preceptors and residents, strengthen our accreditation assessment story, and make it easier for Site Directors to use assessment information with confidence.
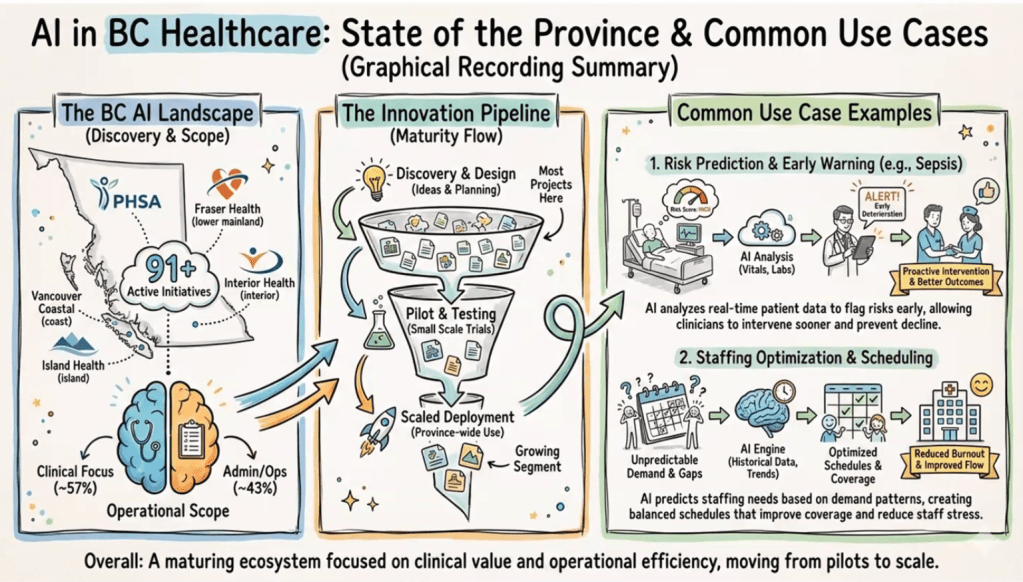
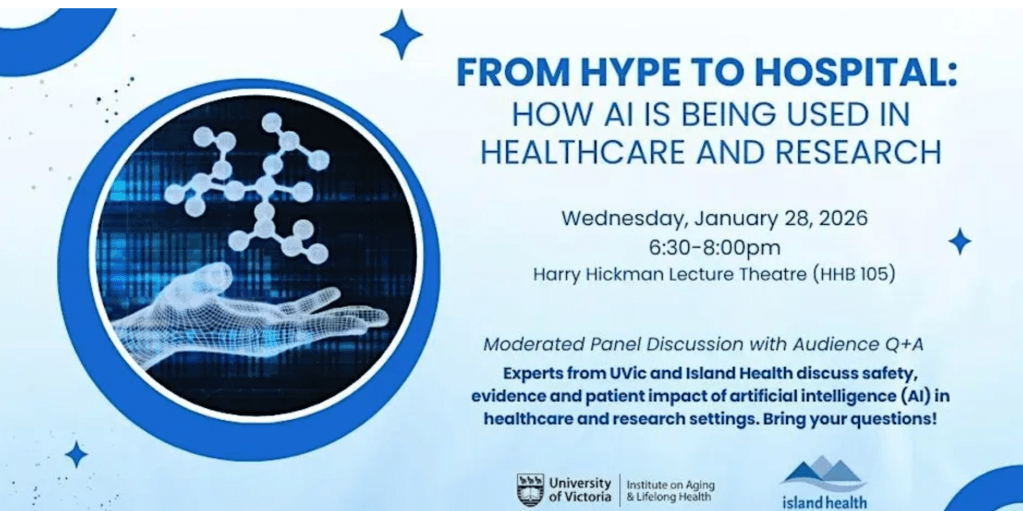
Last night I attended the “From Hype to Hospital: How AI is being used in Healthcare and Research” hosted in British Columbia, Canada.
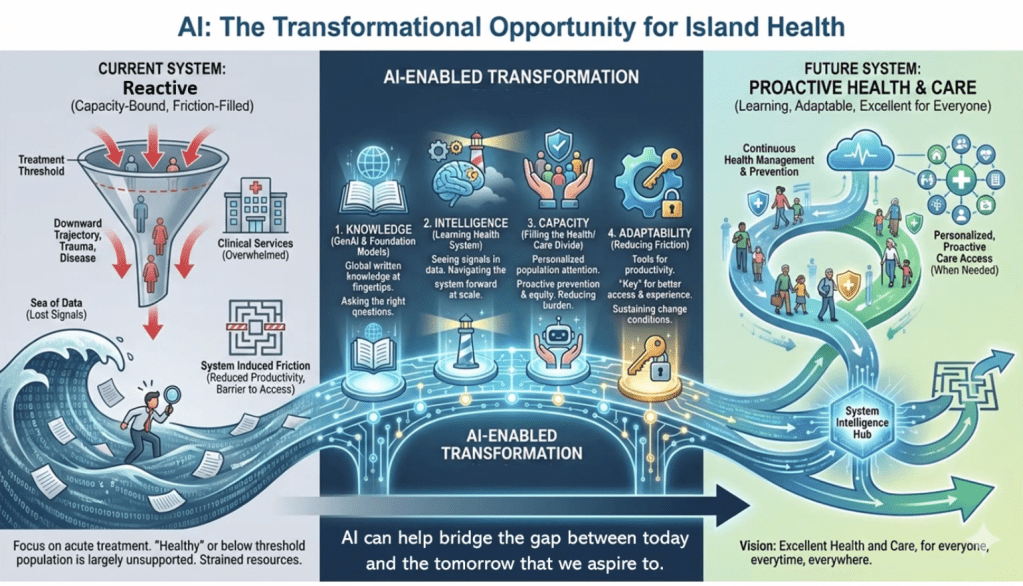
We’re surrounded by data in our healthcare system, but our ability to convert it into timely, trustworthy decisions is still limited by workflow, infrastructure, and governance. Provincial data collection continues to be labour intensive, often manual, and delayed.
As it was reported this evening, in trauma care, there can be a 12-18 month lag between what happens in the Emergency Department and Trauma Service, and what ultimately lands in registries, dashboards, and system-level reports. Check out the article “iROBOT: Implementing Real-time Operational dashBOards for Trauma care” to learn more: https://lnkd.in/gvBQKMgs
Other interesting points from presenters include:
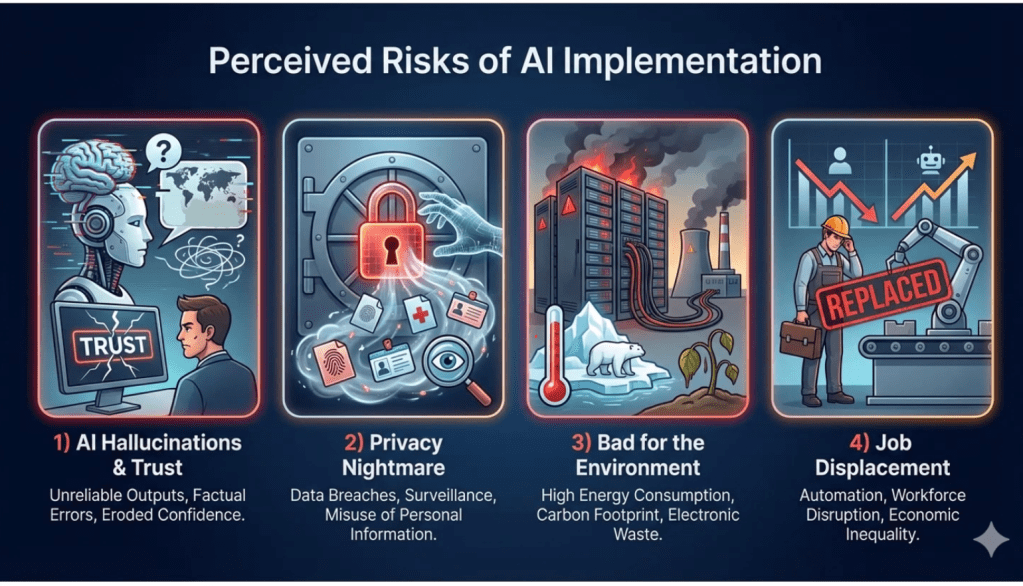
+ Structured data is easy to analyze, narrative data holds the nuance that can change risk and interpretation. + AI can speed screening and reporting, reduce false positives, and support real-time dashboards, if evaluated honestly. + In BC, common use cases are emerging: early warning (sepsis, deterioration), staffing and scheduling, operational intelligence. + The hard part is the pipeline: discovery to pilot to scaled deployment, many projects stall before impact. + Implementation risks are real: trust (confabulation, over-reliance), privacy, environmental cost, workforce disruption.
My takeaway: We have a responsibility to educate and train healthcare practitioners in the use of AI, and to start asking critical questions about how it will affect patient care.
Slides attached are from Graham Payette’s AI BC briefing.
The UBC FP Chilliwack program has invited the Abbotsford-Mission team to join them for their upcoming Preceptor Retreat on Friday, February 27, 2026. I will be leading a session on AI in Faculty Development: Coaching Better Thinking, Strengthening Assessment, and Evaluating the Evaluators. I look forward to seeing you all there!
Please find the “Save the Date” details below and attached for your reference:
Date: Friday, February 27, 2026 Location: Chilliwack (CGH) Participants: Chilliwack & Abbotsford-Mission Postgraduate and Undergraduate Preceptors Schedule:3:00 PM – 6:00 PM: Faculty Development Sessions at CGH 6:00 PM – Late: Dinner and Evening Learning Panels
When Disaster Hits, Family Medicine Is Still the Front Door
Disasters and major trauma can feel like “someone else’s job” until the day your clinic, urgent care, or community hospital becomes the first place people arrive. In those moments, what matters most is not just clinical knowledge, it is teamwork, role clarity, and a shared plan.
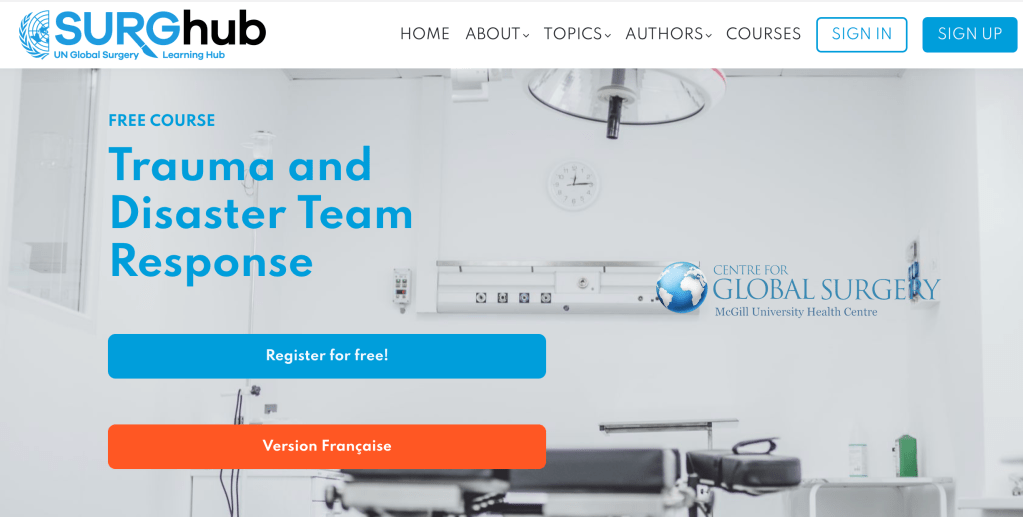
A useful option is Trauma and Disaster Team Response, a free online course on SURGhub, offered through the McGill University Health Centre, Centre for Global Surgery. It is built around multidisciplinary trauma and disaster response, with lectures and quizzes, and it is designed to strengthen how teams function under pressure.
Why it matters for family medicine
Family physicians are often central to stabilization, triage, transfer decisions, and supporting staff and communities in the aftermath. This training can help build a common language for response, especially in rural and community settings where resources and staffing can shift quickly.
What you can take back to your team
Clearer roles during urgent resuscitation and surge situations
More confidence with transfer readiness and escalation
A framework for thinking about disaster response as a system, not just a single patient
A nudge to turn preparedness into practical clinic improvements (call trees, checklists, short drills)
Experts from UVic and Island Health discuss safety, evidence, and patient impact of artificial intelligence (AI) in healthcare and research. Learn more and register here.
To kick off our 2026 Dawn Patrol Faculty Development Series, we’re starting with a topic that hits every exam room, every day. I’ve invited Sean McKelvey, BSc(Pharm) to share practical, evidence-informed insights on how food and lifestyle can meaningfully shift metabolic health, including the big question: can Type 2 diabetes remission be achieved through diet and lifestyle?
I had the opportunity to connect with Sean last year at our Curriculum Retreat, and I thought his presentation was fantastic and incredibly timely given how we’re trying to move in a direction that educates patients on the role of food and nutrients in their overall health.
This faculty development session explores the science and practice of therapeutic nutrition in primary care. Learn evidence-based strategies to support patients in reversing chronic disease through sustainable, food-first approaches.
Session Title: Reversing Chronic Disease in Primary Care: A Food-First Prescription
Speaker: Sean McKelvey, BSc(Pharm), Chief Executive Officer, Institute for Personalized Therapeutic Nutrition (IPTN)
Learning Objectives:
Understand the therapeutic nutrition model and remission criteria
Review evidence and guidelines from Diabetes Canada and ADA/EASD
Explore how interprofessional teams can safely support medication de-escalation
Identify practical resources for patients and health professionals
Event Details:
📅 Friday, January 30, 2026 🕖 07:00–07:45 AM (Pacific Time) 📍 Virtual via Zoom: Email jacqueline.ashby@ubc.ca for link
Who Should Attend: Family physicians, preceptors, residents, nurse practitioners, and allied health professionals interested in integrating therapeutic nutrition into clinical teaching and patient care.
Hosted by: Dr. Jacqueline Ashby, UBC Faculty Development, Team-Based Primary Care Learning Centres (TPCLC)
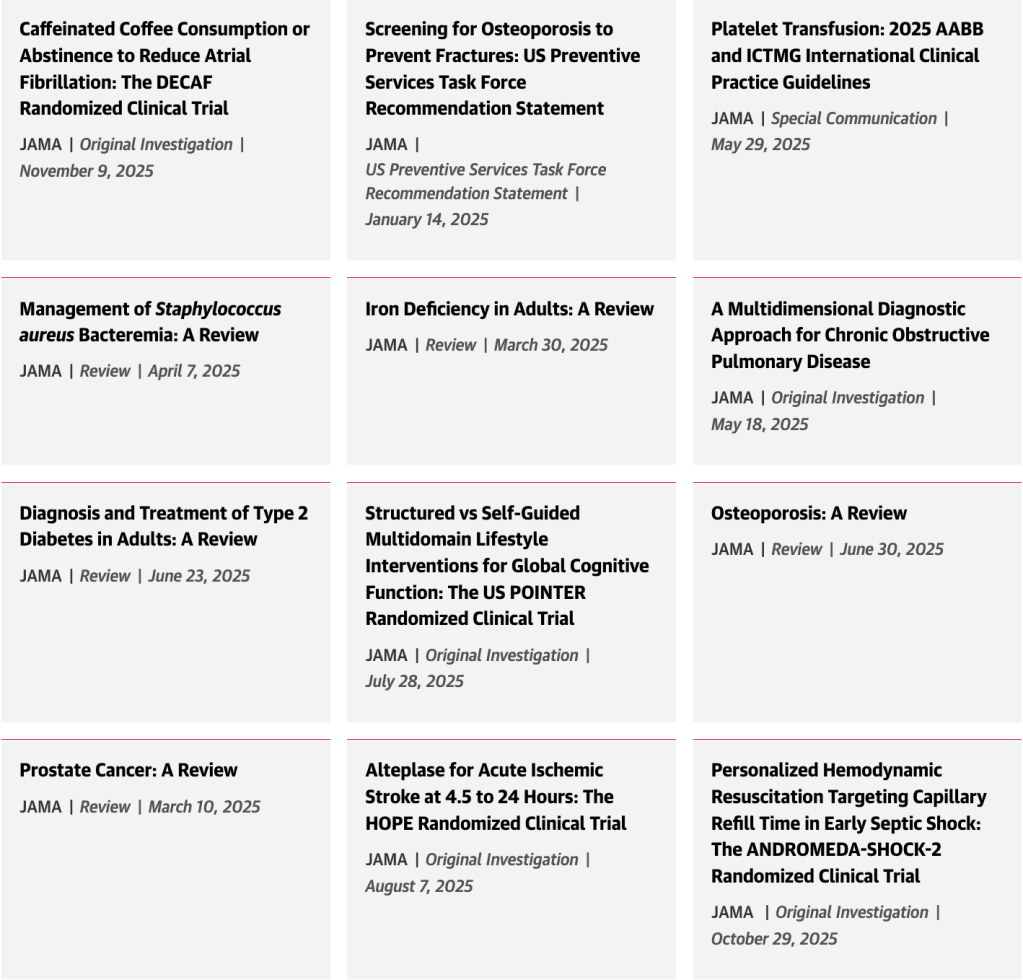
Read the most popular JAMA articles in 2025 including coffee and AFib, osteoporosis, platelet transfusion, type 2 diabetes, S aureus bacteremia, septic shock, and more.
“Delivered through the Nova Scotia Health Authority, the program aims to break down systemic barriers that Black women often face when navigating the health-care system, according to Natalie Johnson, the program’s team lead and registered dietitian.
‘They’re able to come here and let some of those walls down, [be] able to open up about things that they may not be able to open up with a health-care provider who doesn’t get their experience as a Black woman,’ she said.
MacKinnon said she’s working on healing both physically and psychologically from experiences of racism and discrimination she’s endured throughout her life. But within the traditional health-care system, she said clinicians rarely acknowledged how those experiences affected her overall health.”
Read more on How this team is transforming health care for African Nova Scotian women via CBC News.
ABSTRACT: Addressing barriers to cervical cancer screening as a public health priority in British Columbia requires innovative approaches. Community-based health promotion initiatives like Papapalooza connect the public with low-barrier cervical cancer screening and accessible health education, offering inclusive, celebratory, and trauma-informed Pap test experiences through pop-up events.
To determine whether patients support Papapalooza as a strategy to reduce screening barriers, we administered 354 pre-Pap surveys and 309 post-Pap surveys to 533 Papapalooza attendees at five events held between March and June 2023. Identified barriers included inaccessible primary care, provider-related factors, and personal factors. Surveys showed increased knowledge and comfort accessing and understanding the importance of screening, with 93.8% of post-Pap survey participants “very likely” to attend another Papapalooza.
Community-based health promotion is an acceptable means of connecting patients with important screening, while creating meaningful opportunities to enhance health literacy.