
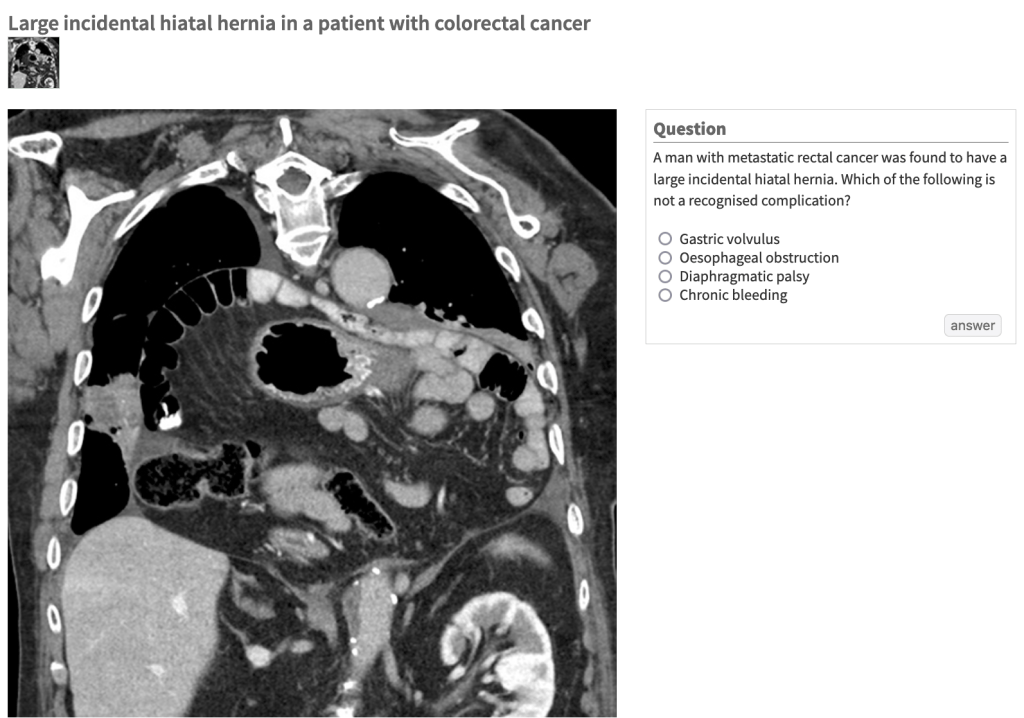
Another round of the Lancet picture quiz! 🙂
“What is…?”
Cue the beat!
Click here to answer.
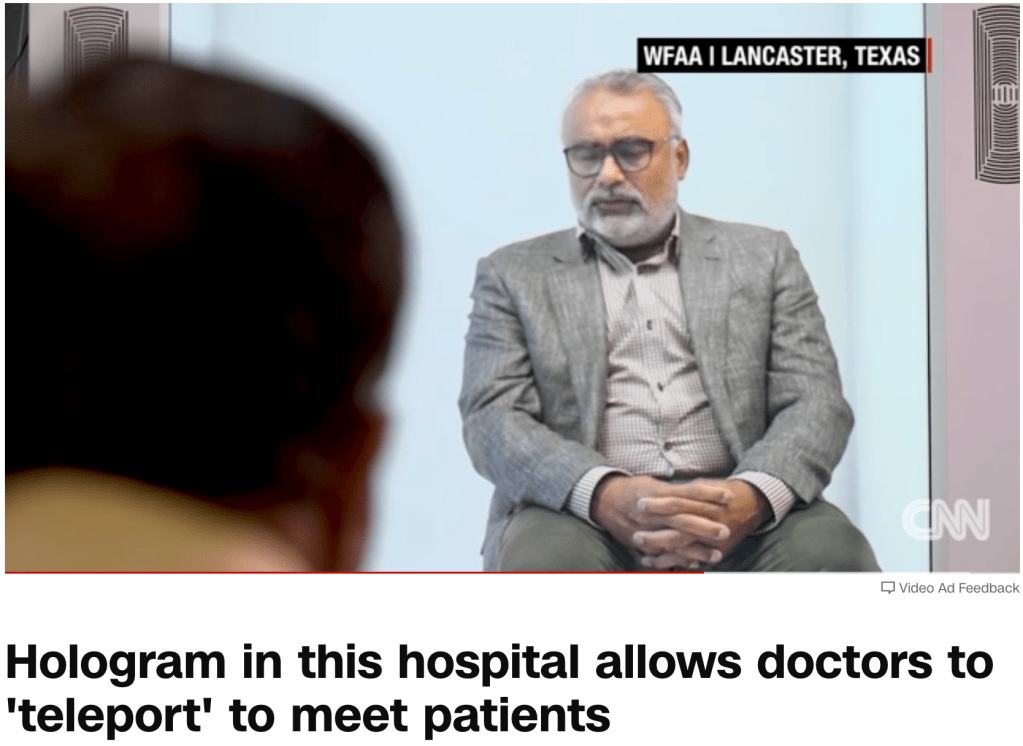
“A newly installed holographic display in Crescent Regional Hospital in Lancaster, Texas, is allowing doctors to meet with patients in real-time and helping them reduce travel time.” CNN affiliate WFAA has more.
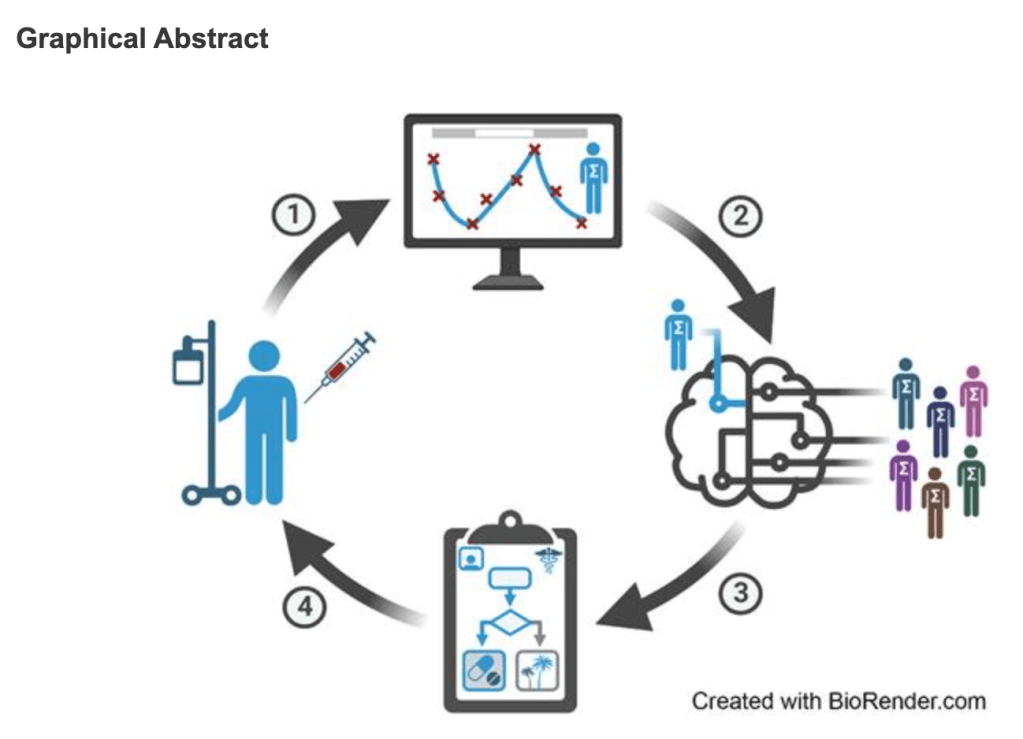
“In a new study published in Cancer Research, researchers from the University of Oxford and Moffitt Cancer Center in Florida introduce a novel framework that applies deep reinforcement learning, DRL, (a form of AI) to create adaptive therapy schedules for individual prostate cancer patients. The results indicate that the new adaptive approach could potentially double the time to relapse compared to MTD or non-personalised treatment breaks.”
Read more on Study demonstrates how AI can develop more personalised cancer treatment strategies via University of Oxford.

“This article addresses the critical issue of violence against children, defined as a violation of their rights across interpersonal, community, societal, and global settings, encompassing both physical and psychological actions targeting them or their parents. Globally, WHO estimates that an unacceptably large number of children aged 2–17 years, experience physical, sexual, or emotional violence or neglect yearly. War stands out as a major contributor to the infringement of children’s fundamental human rights. Those in conflict zones undergo traumatic experiences, including the loss of family members, disruptions to social networks, displacement, and the denial of basic needs. The severe deprivation of essential resources and opportunities, coupled with the stress of warfare, poses a grave threat to the emotional and cognitive development of children, increasing the risk of physical and mental illnesses, disabilities, social problems, and intergenerational consequences. The article aims to draw attention to this issue and advocates for the development of appropriate academic and post-academic educational courses and training programs. This will better equip pediatricians and healthcare professionals to effectively combat violence against children in any context.”
Read more on War inflicts severe violations on the fundamental human rights of children via Global Pediatrics.
Get Cyber Safe is a national public awareness campaign created to inform Canadians about cyber security and the simple steps they can take to protect themselves online. Learn how to secure your accounts, devices, and connections.
Start by taking the Get Cyber Safe Checkup here!
“The Data Science and Health (DASH) Cluster is building a system to link health research data in BC by enhancing the availability and use of health data to improve diagnosis, treatment, and prevention of disease, and enable computational tools that speed discovery of new knowledge, optimizing health outcomes for all BC residents.
The UBC Micro-certificate in Health Data Analytics: Opportunities and Applications is a new program developed by the UBC DASH Cluster and the Data Science Institute for health care professionals and researchers in the health sector with exposure to health data, either clinical or operational. Designed by industry and academic experts, the micro-certificate consists of three four-week online courses, combining self-paced independent study with weekly live online sessions.
In this information session, get an overview of the program, the curriculum, learning outcomes, and what to expect. Meet the program instructors to learn about how you can apply your learning to benefit your organization or your personal endeavours. There will be plenty of time for your questions!”
Learn more via DASH.

“The R21/Matrix-M™ malaria vaccine represents the start of a global effort to eradicate malaria with the addition of vaccine to other measures and highlights Oxford’s commitment to addressing global health challenges in regions heavily affected by the disease.
R21 is the second malaria vaccine to be recommended by WHO for children living in endemic areas. Along with the earlier WHO recommendation of the RTS,S vaccine, there is now many-fold greater vaccine supply for Africa where the disease kills nearly half a million children annually. The rollout of both vaccines is funded by Gavi, the Vaccine Alliance.
Integrating these vaccines into national malaria control plans, along with other interventions, aims to drastically reduce childhood mortality and strengthen the fight against malaria.”
Read more on Shipment of R21 malaria vaccine to Central African Republic marks latest milestone for child survival via University of Oxford.
Learn more about detecting, navigating and discussing health misinformation
June 27 (Thu) | 6:30–8 p.m. PDT | Webinar
Audience: all health professionals
Overview: Gain insight on how to help patients navigate health misinformation and get access to recommended resources to help clinicians and patients assess the reliability of health information. Our panellists are available to share their knowledge and experience — don’t miss this opportunity to get your questions answered. Learn more here.
Up to 1.5 Mainpro+/MOC Section 1 credits
Hello Team! I wanted to introduce you to a series of free online modules focused on community engagement and involvement in global health research. This course was designed by Dr. Alun Davies, a Research Fellow at Green Templeton College, University of Oxford. “The aim of this course is to develop learners’ understanding and knowledge of CEI, supporting their ability to plan and design ethical and impactful CEI in health research. For the purposes of this course, we use the term CEI to mean:
‘An active involvement of the community throughout the research process, using participatory approaches and working in partnership with all key stakeholders. CEI includes a range of activities which involve interactions between researchers, community members and stakeholders, aimed at improving the relevance, value and conduct of health research.’
In progressing through the modules, learners will gain a better understanding and appreciation of the terms used for CEI, the broad range of CEI aims and approaches, and the overall value of CEI. CEI is an essential and rewarding component of research, and, as the course authors, we hope that you enjoy learning about it through this course.
The 7 course modules have been authored and peer reviewed by specialists in the area of CEI.
Who is this course for?
This course is open to all with an interest in CEI in health research including:
Course learning outcomes:
Learners completing this course will be able to:
How to use the course:
The different modules of the course can be undertaken in any order. After successful completion of each end-of-module quiz, a certificate can be obtained. Alternatively, depending on your needs, you can select individual modules to complete.
Certification:
An electronic certificate of completion can be obtained for each module once the corresponding module quiz is completed. You will need to score 80% or more to receive a certificate.
Learn more via The Global Health Network MESH.
Best,
Jacqueline

The Impact of AI in Health Research: Transforming Career Trajectories
June 10, 2024, 12:00 pm to 1:30 pm
Looking for artificial intelligence (AI)-related opportunities in academia or industry? Join the VCHRI Trainee Committee for an insightful exploration of how professionals utilize AI to advance health research and enhance health care delivery.
An expert panel of speakers will share their experiences, addressing misconceptions and answering questions. Pizza and light refreshments will be provided.
Event is in-person at Paetzold Auditorium, Vancouver General Hospital.
About the speakers:
